

A recent study published in BMJ Open highlighted the EVA System Colposcope in performing Digital Colposcopy (DC) on hrHPV+ women in Cambodia. With a shortage of trained gynecologists in Cambodia, DC can be performed by trained nurses or midwives. According to the study, images obtained with the EVA System “have excellent resolution and can be easily magnified to visualise morphological feature consistent with high dysplasia such as mosaicism and punctation (figure 2).” They additionally noted that the digital images can be used in continuing education and quality control for nurses and midwives and that the digital images can be shared securely in a cloud-based portal for real-time consultation by an expert colposcopist in Cambodia or worldwide.
READ THE ORIGINAL ARTICLE>OBJECTIVES: Logistical and economic issues make traditional cytology-based cervical cancer screening challenging in developing countries. Alternative, cost-effective screening strategies must be developed to screen millions of women in resource-poor countries such as Cambodia.
DESIGN: A prospective cohort study during which all women underwent four cervical cancer screening methods: (1) self-sampled human papilloma virus (HPV) testing (careHPV system), (2) clinician-collected HPV testing, (3) visualization with acetic acid (VIA), and (4) digital colposcopy (DC) with the Enhanced Visual Assessment System (EVA).
SETTING: A referral hospital in Phnom Penh, Cambodia.
PARTICIPANTS: Two hundred and fifty Cambodian women (129 HIV+, 121 HIV-). Subjects were recruited from the National Center for HIV/AIDS Dermatology and sexually transmitted disease (STD) cohort, the Sihanouk Hospital Center of Hope’s Rural Outreach Teams, and the Pochentong Medical Center.
RESULTS: Fifty-six of the 250 (22.4%) patients tested positive for high-risk HPV (hrHPV+). Thirty-seven of the 129 HIV+ women were hrHPV+ (28.6%), whereas 19 of 121 HIV- women were hrHPV+ (15.7%) (p=0.0154). Self-sampling HPV specimens identified 50/56 (89%), whereas physician-collected specimens identified 45/56 (80%) (p=0.174). 95.2% of patients felt comfortable obtaining HPV self-samples. Thirty-seven of 250 women were VIA+. Thirty of 37 VIA+ women underwent confirmatory biopsies for cervical intraepithelial neoplasia (CIN) (26 CIN1, 4 CIN2+). The rate of confirmed dysplasia in the HIV+ group was 20/129 (15.5%) compared with 10/121 (8.26%) in HIV- women (p=0.0291). The contemporaneous physician impressions of the DC images accurately differentiated between CIN1 and CIN2+ lesions in all 30 women having confirmatory biopsies.
CONCLUSIONS: The results of this study suggest potential modifications of the current cervical screening strategy that is currently being employed in Cambodia. The first step in this new strategy would be self-swabbing for hrHPV. Subsequently, hrHPV+ patients would have DC and immediate treatment based on colposcopic findings: cryotherapy for suspected CIN1 and loop electrosurgical excision procedure (LEEP) for suspected CIN2+.
Thay S, Goldstein A, Goldstein LS, et al. Prospective cohort study examining cervical cancer screening methods in HIV-positive and HIV-negative Cambodian Women: a comparison of human papilloma virus testing, visualization with acetic acid and digital colposcopy. BMJ Open 2019;9:e026887. doi: 10.1136/bmjopen-2018-026887

(NOTE: Using the EVA System to visualize and document the instruction with the cervical cancer instructional apparatus.)
BACKGROUND: Cervical cancer remains one of the leading causes of cancer for women in medically underserved areas. This is in part due to a lack of trained clinicians to provide the necessary diagnosis and treatment of precancerous lesions to prevent cervical cancer. Increasing medical provider knowledge and skills is important for the early detection and prevention of cervical precancer and cancer in medically underserved areas of the United States and globally.
METHOD: LUCIA is a low-cost, universal cervical cancer instructional apparatus that can be used to teach and practice a variety of essential skills for cervical cancer screening, diagnosis, and treatment, including: visual inspection with acetic acid, Pap and human papillomavirus DNA specimen collection, colposcopy, endocervical curettage, cervical biopsy, cryotherapy, and loop electrosurgical excision procedure.
EXPERIENCE: LUCIA was used to provide hands-on training in six courses held in Texas (n=3), El Salvador (n=1), and Mozambique, Africa (n=2). Standardized provider evaluations were administered at three of these courses and resulted in mean scores of 4.12/5 for usefulness, 4.46/5 for skill improvement, and 4.43/5 for ease of skill evaluation.
CONCLUSION: LUCIA provides dynamic, real-time feedback that allows trainees to learn and practice important skills related to cervical cancer prevention while simulating a patient exam.

Objective: To evaluate the acceptability and safety of thermal ablation (TA) for the treatment of precancerous cervical lesions in women in Honduras.
Initial Lessons From Implementing a Telecolposcopy Program on a High Risk Population in California from MobileODT
Rachel Steward (1), Jennifer Spohn (1), Eliya Tenenboim (2), Cathy Sebag (2), David Levitz (2)
(1) FPA Women’s Health, Los Angeles, CA (2) MobileODT, Tel Aviv, Israel
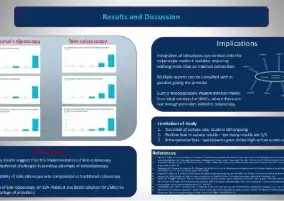
Objective: To assess the feasibility of a live, telecolposcopy system in clinics serving high-risk populations. Of interest was understanding the feasibility of an integrated telecolposcopy solution from the perspectives of patient and provider acceptance in comparison to in-person oversight of an exam.
Methods: A custom feature was built into MobileODT’s EVA System, a smartphone-based colposcope, utilizing a video-conferencing application. Through screen sharing, the point-of-care provider shared a live video feed of the colposcopy exam with a remote expert, who then recommended biopsy sites. Following the procedure, satisfaction surveys were administered to all remote experts, point-of-care providers, and patients. All twelve subjects who underwent telecolposcopy completed surveys. As a control group, 10 patients undergoing traditional colposcopy were also surveyed.
Results: Initial findings showed that experts were able to assist junior providers during colposcopy procedures. Patients reacted positively to live expert supervision.
Conclusions: Preliminary results suggest that live telecolposcopy is feasible on a mobile, connected colposcope.

Cervical intraepithelial neoplasia (CIN) can be treated with surgical excision or ablation methods. Loop electrosurgical excision procedure (LEEP), the most commonly used excision treatment in high-resource settings, involves surgical removal of the squamocolumnar junction (SCJ) using a wire loop with a high-frequency electric current.

Objectives: To provide a systematic review of cold coagulation efficacy and acceptability for cervical intraepithelial neoplasia (CIN) treatment through a meta-analysis of clinical reports and a randomized controlled trial.

Objective: A prospective randomized study is presented of 161 patients with cervical intraepithelial neoplasia.